Macular Degeneration


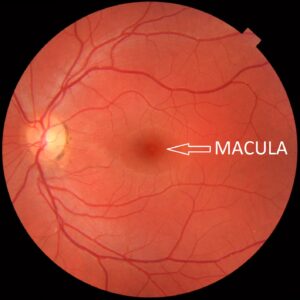
What is the Macula?
This is a small area of your retina (the “film” layer) at the back of your eye that is responsible for your central vision. It consists of a small pit (the fovea) containing an extremely high concentration of the high resolution and colour sensitive cone photoreceptor cells.
Age Related Macular Degeneration (AMD)
- This disease results in the degeneration of the maculae, and thus, loss of central vision.
- When cells in the body gain energy from nutrients they produce toxic waste known as free radicals or oxidants. These free radicals result in oxidation and damage to the cells, which in turn trigger a cascade of inflammatory processes.
- This process holds true in the eyes too. The retinal pigmented epithelium is a layer of the retina responsible for clearing waste products from the retina. If this layer cannot do this well the waste products build up and form white/yellow deposits called Drusen – the hallmark of Macular degeneration. These drusen then block nutrition getting to the overlying cells in the retina resulting in progressively poorer central vision.
- There are 2 types of AMD; Dry and Wet

Dry AMD
- This form is characterised by drusen that gradually disrupt central vision.
- This form of the disease progresses more slowly. However, there is no current cure for it. A good diet (rich in anti-oxidants), supplements, and a healthy lifestyle can help slow the progression.
- Dry AMD can eventually lead to much more widespread damage to the macula, termed geographic atrophy
Wet AMD
- About 10-20% of people with dry AMD will progress to the wet form of the disease, which can cause much more destruction of the retina, particularly if it is not treated promptly.
- One of the inflammatory processes that can occur in the eye in an effort to help with the oxidative stresses is to develop new blood vessels to deliver oxygen and nutrients to the damaged macula cells. However, these blood vessels are abnormal, weak and leaky.
- The blood and protein leakage from these abnormal vessels results in retinal bleeding and swelling if left untreated. This leads to distortion of the vision and ultimately loss of vision.
Treatment
- It is important to know that there are no cures for the disease but we can aim to slow the progression of vision loss and sometimes improve the vision.
- There are no approved treatments available for the dry form of the disease in Australia. However, there are several treatment trials throughout Australia and abroad that are currently underway, involving various techniques including laser treatment and other medications.
- Once new blood vessels develop, there are treatments available that aim to inhibit the growth of these vessels.
- In the past, laser treatment to the affected areas was the predominant treatment to seal these abnormal vessels off. This is now reserved only if other treatments are not successful.
- Injections of medicines that inhibit the blood vessel growth is the primary and most successful treatment available. Your ophthalmologist will organise a schedule for when to deliver the injections depending on each individual’s presentation and response to the injections. Injections are typically administered more frequently at the beginning.
- Low vision aids can be prescribed to provide better vision for people with macular degeneration. See this article for more information >> Low Vision Aids article
A healthy diet and lifestyle can make all the difference

Healthy Diet
- Lutein and Zeaxanthin: Dark green leafy vegetables and fresh fruit are great sources of the antioxidants Lutein and Zeaxanthin, which are depleted in people with poor macula health. As a general rule, the darker the green, the higher the lutein, so this includes spinach, silver beet, collard greens and especially kale
- Omega-3 fatty acids: Fish/seafood 2-3 times a week will increase your Omega-3 intake which is important for eye health. Particularly oily fish, such as salmon, anchovies, sardines etc.
- Zinc: Oysters, seafood, nuts and legumes o Vitamin C: citrus fruits, berries and tomatoes
- Vitamin E: nuts and whole grains o Selenium: nuts (Brazil nuts in particular)
- Low GI carbohydrates: evidence suggests that people that consume low GI carbohydrates (fruit, vegetables, whole grain cereals/breads and legumes) reduce the risk of developing macular degeneration compared to those consuming more high GI foods.
Vitamin supplements
- The Age-Related Eye Disease Study 2 (AREDS-2) found that in people diagnosed with AMD, a special formula of supplements slowed the progression from intermediate to advanced AMD by 25%.
- The AREDS2 formula is made up of:
- Vitamin C 500mg, Vitamin E 400iu, Lutein 10mg, Zeaxanthin 2mg, Zinc 80mg, Copper 2mg
Cessation of smoking:
- This is the largest modifiable risk factor for AMD – smoking can increase your risk by three fold.
Physical activity:
- Various studies have supported this inverse relationship. One study (*) showed that people that engaged in high metabolic energy activities throughout the week were 54% less likely to have early AMD.
Sunglasses
- These provide adequate protection from UV light, as well as limiting the increased glare and decreased contrast sensitivity that AMD sufferers can experience.
Regular eye checks for everyone.
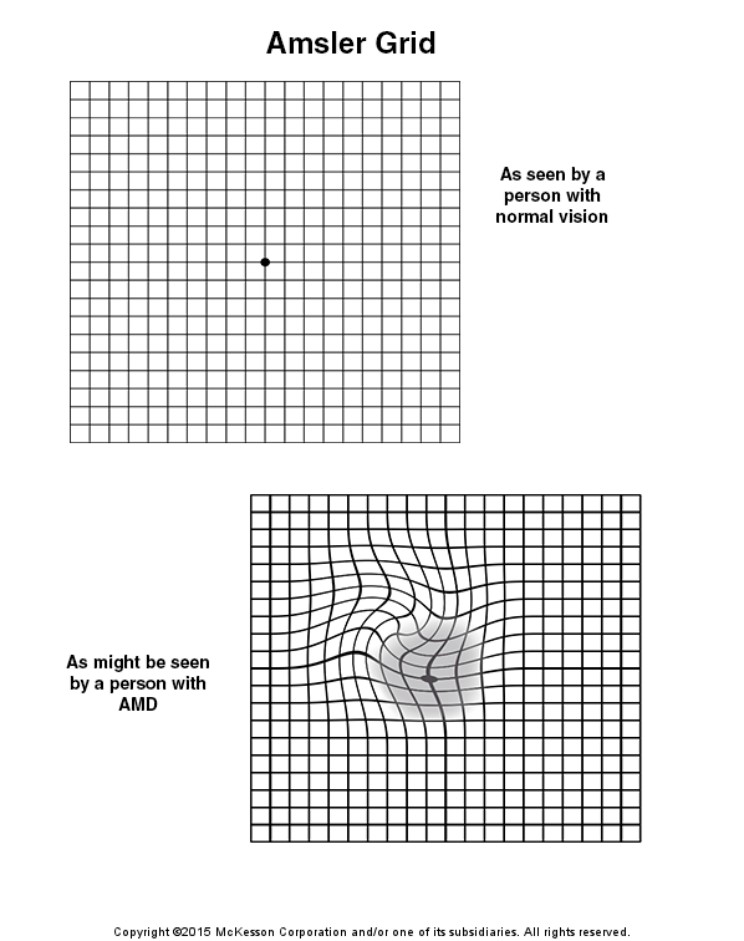
Amsler grid checks
- Amsler checks should be done regularly for those with AMD to monitor symptoms at home. With your reading glasses, cover one eye and look at the black spot. Are any of the lines distorted? Any of the boxes or corners of the grid missing? Any black patches in your vision? If there are any changes, return to the clinic as soon as you can.
Social and psychological effects
- Although AMD is a physical disease, there are several psychological effects that sufferers can experience and it can really impact a sufferer’s daily life and quality of life.
- Low vision can prevent people from partaking in activities that we would normally take for granted, such as driving, reading, watching TV, and working.
- Getting around can be a lot harder so sufferers may choose to stay at home more. Some people may fear the idea of having a cane or walking stick to help get around because they think people will label them as blind. This may further limit their excursions outside their home.
- Patients can get very upset about the burden they put on family members having to drive them around, including to and from appointments.
- The idea of having intra-ocular injections can create great anxiety in certain individuals.
- One of the least talked about issues that can result from significant vision loss, particularly in AMD, is Charles Bonnet Syndrome. This is where mentally healthy people experience vivid visual hallucinations when they are in low stimulating environments – this can obviously be quite distressing to patients and they often do not discuss it with family or health professionals because they don’t want people to think they have mental health issues. The hallucinations can be complex (and sometimes bizarre) patterns or images of people, animals or inanimate objects. Studies suggest that as many as 30% of people with significant vision loss experience these hallucinations. The underlying mechanism for this is not well understood and there are no cures. However, there seems to be a relationship between these hallucinations occurring in environments where people are deprived of sensory stimulation, e.g. dim and familiar rooms. Thus, encouraging more ventures outside and social activities will reduce the occurrence of these hallucinations. Also, discussing your symptoms with people (family, friends, doctors) seems to reduce the frequency of hallucinations. The hallucinations tend to cease after about 12-18 months.
The Macular Degeneration Foundation offers many resources that you can order and get sent to your home. Click here to get sent to their website for more information.
*https://www.ncbi.nlm.nih.gov/pubmed/21149749
**https://www.mdfoundation.com.au/


